MeiboVue in Sjögren's Dry Eye: Tracking Severe Gland Dropout When Symptoms Improve
You finish a follow-up visit in a patient with Sjögren's-associated dry eye. They report better comfort. Corneal staining has improved. Scleral lenses are working. Then the practical question returns: did severe meibomian gland dropout stay stable, or is it progressing — and how do you document that conversation?
Symptom scores and staining maps answer part of the story. They rarely show patients what severe dropout looked like at baseline or whether repeat meibography suggests stability across visits. In advanced meibomian gland dysfunction, that gap matters: patients may feel improvement while gland morphology remains severely compromised — and clinicians still need longitudinal records that support monitoring, not only reassurance.
MeiboVue is a portable handheld meibography system for dry-eye screening, baseline documentation, patient education, and follow-up comparison in pre-test or chairside flow. Imaging supports documentation and education. It does not replace your examination, treat gland dropout, imply gland regrowth, or substitute for standard dry-eye assessment and clinical judgment.
Why Follow-Up Meibography Is More Than a Baseline Snapshot
In severe autoimmune dry eye, baseline meibography often documents pronounced dropout — especially on the lower lids. That image can help set realistic expectations when patients first hear "MGD is severe."
What changes at follow-up is the comparison question:
- Did symptoms and ocular surface signs move in a direction you expected?
- On repeat imaging, does visible gland morphology appear stable, worsening, or changing?
- Can you show the patient both time points on screen — without overstating what imaging proves?
Most lanes do not have a fixed desktop meibographer at every dry-eye revisit. Teams that want structured gland documentation in normal flow may benefit from portable capture at baseline and again at follow-up.
✓Portable meibography: Handheld capture supports meibomian gland imaging in pre-test or chairside flow without dedicated room infrastructure.
✓Voice-activated capture: Hands-free imaging during lid manipulation may shorten operator friction in busy dry-eye workflows.
✓Patient education: Visible gland morphology can help patients understand why lid care, thermal therapy, anti-inflammatory steps, or closer follow-up may be recommended.
✓Baseline plus follow-up compare: Store baseline and repeat captures to discuss symptom change and visible gland findings across visits.
✓Longitudinal tracking: Repeat meibography may support disease-course documentation when severe dropout is already present — without implying treatment regrowth from imaging alone.
Case Walkthrough: Severe Dropout, Multimodal Care, Stable Morphology on Repeat Imaging
The following de-identified case comes from a clinician-provided summary. Images show visible findings for education and longitudinal tracking — not standalone proof of treatment effect from meibography.
Presentation and Baseline Findings
A 32-year-old male with Sjögren's syndrome presented with chronic dry eye symptoms. Despite initial lid hygiene, lubricants, and anti-inflammatory therapy, symptoms and ocular surface signs persisted.
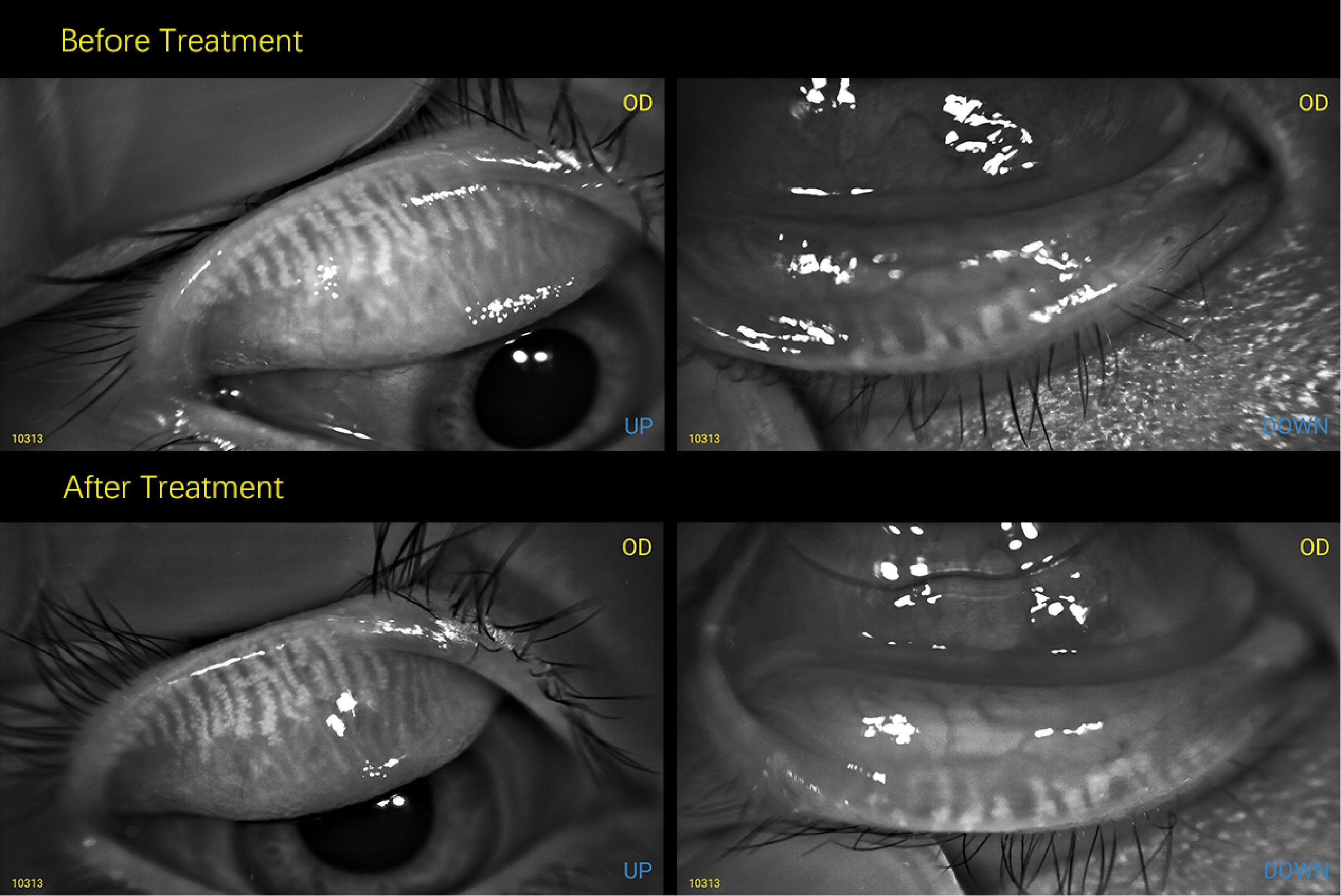
Baseline examination demonstrated severe evaporative dry eye with significant meibomian gland dysfunction. Clinical signs included conjunctival injection, reduced tear stability, and corneal staining. Bilateral four-lid MeiboVuemeibography documented severe gland dropout, with pronounced loss visible on the lower lids — particularly OS lower (Dec 2024).
In advanced MGD, baseline meibography may help clinicians document dropout severity, frame realistic expectations, and establish a visual record before escalating multimodal care.
Management
The patient was managed with a clinician-directed multimodal approach:
- IPL for severe MGD and evaporative dry eye
- Ikervis (ciclosporin) as ongoing anti-inflammatory therapy
- Scleral lens fitting for ocular surface protection and comfort when symptoms and surface disease persisted
Treatment decisions and outcomes remain with the examining clinician. MeiboVuedocuments visible gland morphology; it does not deliver therapy.
Follow-Up: Symptoms, Staining, and Repeat Meibography
At follow-up, the patient reported improved comfort and was wearing scleral lenses with minimal symptoms. Ocular surface staining had improved, with minimal to no corneal staining noted on examination. Ikervis and scleral lens wear continued as part of ongoing dry-eye management.
On repeat meibography (Apr 2026), no visible progression of gland dropout was observed — morphology appeared stable between visits on the compared lower-lid capture. That finding supports a qualified clinical narrative: symptom and surface improvement alongside stable visible gland morphology on imaging — not gland regrowth or reversal of dropout from the camera or from imaging alone.
This is where portable follow-up meibography may add value: pairing how the patient feels with what repeat imaging shows when dropout was severe at baseline.
The case supports:
- Baseline documentation of severe dropout in Sjögren's-associated dry eye
- Qualified follow-up outcomes (reported comfort, staining improvement noted on examination)
- Before/after meibography comparison framed as longitudinal tracking
- Discussion of whether severe dropout appears stable or progressing across visits
Three Steps in a Baseline-Plus-Follow-Up Meibography Workflow
- Capture baseline — four-lid meibography at dry-eye workup or MGD intake; review with the patient on screen; store per clinic policy.
- Manage per your protocol — lid care, thermal therapy, IPL, pharmacologic therapy, specialty lenses, and follow-up intervals remain clinician-directed.
- Repeat and compare — at follow-up, recapture matched lids; discuss symptom change alongside whether visible morphology appears stable, worsening, or changing.
This workflow fits teams that already discuss MGD verbally but want a repeatable visual record for education, staff training, and longitudinal review.
Request a demo or starter evaluation through your regional VisuScience contact or email info@visusience.com .
Learn more at www.visuscience.com
You finish a follow-up visit in a patient with Sjögren's-associated dry eye. They report better comfort. Corneal staining has improved. Scleral lenses are working. Then the practical question returns: did severe meibomian gland dropout stay stable, or is it progressing — and how do you document that conversation?
Symptom scores and staining maps answer part of the story. They rarely show patients what severe dropout looked like at baseline or whether repeat meibography suggests stability across visits. In advanced meibomian gland dysfunction, that gap matters: patients may feel improvement while gland morphology remains severely compromised — and clinicians still need longitudinal records that support monitoring, not only reassurance.
MeiboVue is a portable handheld meibography system for dry-eye screening, baseline documentation, patient education, and follow-up comparison in pre-test or chairside flow. Imaging supports documentation and education. It does not replace your examination, treat gland dropout, imply gland regrowth, or substitute for standard dry-eye assessment and clinical judgment.
Why Follow-Up Meibography Is More Than a Baseline Snapshot
In severe autoimmune dry eye, baseline meibography often documents pronounced dropout — especially on the lower lids. That image can help set realistic expectations when patients first hear "MGD is severe."
What changes at follow-up is the comparison question:
- Did symptoms and ocular surface signs move in a direction you expected?
- On repeat imaging, does visible gland morphology appear stable, worsening, or changing?
- Can you show the patient both time points on screen — without overstating what imaging proves?
Most lanes do not have a fixed desktop meibographer at every dry-eye revisit. Teams that want structured gland documentation in normal flow may benefit from portable capture at baseline and again at follow-up.
✓Portable meibography: Handheld capture supports meibomian gland imaging in pre-test or chairside flow without dedicated room infrastructure.
✓Voice-activated capture: Hands-free imaging during lid manipulation may shorten operator friction in busy dry-eye workflows.
✓Patient education: Visible gland morphology can help patients understand why lid care, thermal therapy, anti-inflammatory steps, or closer follow-up may be recommended.
✓Baseline plus follow-up compare: Store baseline and repeat captures to discuss symptom change and visible gland findings across visits.
✓Longitudinal tracking: Repeat meibography may support disease-course documentation when severe dropout is already present — without implying treatment regrowth from imaging alone.
Case Walkthrough: Severe Dropout, Multimodal Care, Stable Morphology on Repeat Imaging
The following de-identified case comes from a clinician-provided summary. Images show visible findings for education and longitudinal tracking — not standalone proof of treatment effect from meibography.
Presentation and Baseline Findings
A 32-year-old male with Sjögren's syndrome presented with chronic dry eye symptoms. Despite initial lid hygiene, lubricants, and anti-inflammatory therapy, symptoms and ocular surface signs persisted.
Baseline examination demonstrated severe evaporative dry eye with significant meibomian gland dysfunction. Clinical signs included conjunctival injection, reduced tear stability, and corneal staining. Bilateral four-lid MeiboVuemeibography documented severe gland dropout, with pronounced loss visible on the lower lids — particularly OS lower (Dec 2024).
In advanced MGD, baseline meibography may help clinicians document dropout severity, frame realistic expectations, and establish a visual record before escalating multimodal care.
Management
The patient was managed with a clinician-directed multimodal approach:
- IPL for severe MGD and evaporative dry eye
- Ikervis (ciclosporin) as ongoing anti-inflammatory therapy
- Scleral lens fitting for ocular surface protection and comfort when symptoms and surface disease persisted
Treatment decisions and outcomes remain with the examining clinician. MeiboVuedocuments visible gland morphology; it does not deliver therapy.
Follow-Up: Symptoms, Staining, and Repeat Meibography
At follow-up, the patient reported improved comfort and was wearing scleral lenses with minimal symptoms. Ocular surface staining had improved, with minimal to no corneal staining noted on examination. Ikervis and scleral lens wear continued as part of ongoing dry-eye management.
On repeat meibography (Apr 2026), no visible progression of gland dropout was observed — morphology appeared stable between visits on the compared lower-lid capture. That finding supports a qualified clinical narrative: symptom and surface improvement alongside stable visible gland morphology on imaging — not gland regrowth or reversal of dropout from the camera or from imaging alone.
This is where portable follow-up meibography may add value: pairing how the patient feels with what repeat imaging shows when dropout was severe at baseline.
The case supports:
- Baseline documentation of severe dropout in Sjögren's-associated dry eye
- Qualified follow-up outcomes (reported comfort, staining improvement noted on examination)
- Before/after meibography comparison framed as longitudinal tracking
- Discussion of whether severe dropout appears stable or progressing across visits
Three Steps in a Baseline-Plus-Follow-Up Meibography Workflow
- Capture baseline — four-lid meibography at dry-eye workup or MGD intake; review with the patient on screen; store per clinic policy.
- Manage per your protocol — lid care, thermal therapy, IPL, pharmacologic therapy, specialty lenses, and follow-up intervals remain clinician-directed.
- Repeat and compare — at follow-up, recapture matched lids; discuss symptom change alongside whether visible morphology appears stable, worsening, or changing.
This workflow fits teams that already discuss MGD verbally but want a repeatable visual record for education, staff training, and longitudinal review.
Request a demo or starter evaluation through your regional VisuScience contact or email info@visusience.com .
Learn more at www.visuscience.com